Understandings of testicular cancer in young adult males: A Q-methodological study
Ian Garner[1] , School of Social Science and Law, Teesside University
Abstract
This study used Q-methodology in order to explore the diverse range of meanings and understandings that young males construct in relation to testicular cancer (TC). Using conventional methods of Q-sorting, twenty-seven males aged 18 to 43 sorted a number of statements along a continuum from 'strongly disagree' to ' strongly agree'. Statements represented a wide range of viewpoints concerning the risk factors, causes and symptoms of TC, popular ideas and myths about TC, and the emotional consequences of TC. Centroid factor analysis of the 27 completed Q-sorts revealed four distinct perspectives. The four factors are interpreted and discussed relative to the current research position concerning the negative influence of masculine values on men's testicular-screening behaviours. These four accounts were labelled: Media Influenced, Knowledgeable, Cautious and Mislead. The four perspectives contained different accounts concerning the causes and symptoms of TC, yet participants representing each perspective were unanimous in endorsing testicular self-examination (TSE). Results indicate that young males were more likely to have heard of TC and TSE in comparison to previous studies assessing knowledge of the disease and self-screening practices. Comment is made on the potential implications for public health awareness, and limitations to the study are acknowledged.
Keywords: Testicular cancer, testicular self-examination, health education, Q-methodology, masculinity
Introduction
Testicular cancer (TC), despite being a relatively rare disease, is the most frequently occurring malignancy in males aged 15 to 45 (NHS Choices, 2010). TC accounts for 1% to 2% of all cancers occurring in males, with approximately 2,000 new cases diagnosed in the UK each year (Cancer Research UK, 2010). Incidence rates have risen steadily over the course of the last 30 years; however, the reason for this rise remains unclear (Everyman, no date). Similar increases in TC incidence rates have been reported in numerous industrialised European countries, notably Spain and Slovenia, while overall rates of TC have remained exceptionally high, but stable, in Switzerland for several decades (Bray et al., 2006). In contrast, TC is practically unheard of in parts of Africa and Asia (NHS Choices, 2010). As before, the underlying causes in these trends have not been identified.
Early diagnosis is considered crucial in the successful treatment of TC (Richie, 1993). Delayed detection often results in treatment problems and poor prognosis due to the higher stage of disease at diagnosis (Boyle et al., 1987). Initiatives aimed at reducing diagnostic delay have centred their attention on improving uptake of testicular self-examination (TSE) (Gascoigne et al., 1999). The adoption of TSE as a means of detecting TC is based on the assumption that testicular lumps, swellings and areas of thickness are the most common symptoms associated with TC, and that detection of these symptoms will prompt men to seek medical advice (Gascoigne et al., 1999). TSE is a painless self-screening process, which is considered easy to learn and perform, and encourages males to take responsibility for their own health (Rudberg et al., 2005).
Many attempts have been made to increase awareness of TC amongst male populations (Evans et al., 2006). These efforts have included the publication of leaflets and guides, informational CD-ROMs/DVDs and national media campaigns advocating TSE. Cancer support organisations encourage TSE practice, with advice to seek medical attention should any concerns arise (Handy and Sankar, 2008). While TSE is often recommended, there is surprisingly little data available concerning the prevalence of TC knowledge among male populations. Still, research conducted since the mid-1980s has consistently demonstrated that young males are uninformed about TC and rarely practice monthly TSE in line with recommendations.
In what is now one of the most frequently cited papers in the literature, researchers Goldenring and Purtell (1984) surveyed knowledge and practice of cancer self-screening techniques amongst a sample of US College athletes aged 18 to 23 years. Eighty-seven per cent of males in the sample were unaware of their risk for TC, while only 10% had been taught how to perform TSE. Rather worryingly, only 4% of males in the sample had been taught how to perform TSE by their GP, despite the fact that 97% had undergone a physical examination at some time during the preceding three years. Only 6% of male participants actually examined themselves on a regular basis. Similarly, Moore and Topping (1999) surveyed knowledge of TC and TSE in a sample of 203 male students aged 18 to 45 years, reporting that 32% had prior knowledge of TSE, while only 23% claimed to practice TSE once per month as recommended. While 27% of participants correctly identified the many risk factors and causes associated with TC, 7% felt that sexually transmitted diseases increased TC risk, with a further 2% indicating that HIV was a causal factor. Consistent with these findings, 27% of males in a sample of Swedish high school students indicated that sexual problems were the most common symptom of TC, while only 12% reported having performed TSE during the 12 months previous (Rudberg et al., 2005). Less than half of the participants in the sample (48%) knew that TC was the most common malignancy in their age group. More recently, the work of researchers Güleser and Unalan (2010) and Ugurlu et al. (2010) has added further weight to the notion that young males are misinformed about their risk for TC, and do not understand the importance of periodic TSE.
The low levels of TC knowledge demonstrated throughout these studies is particularly worrying, especially when one considers that males in academia are arguably better educated than peers in other sections of society (Moore and Topping, 1999). Nevertheless, it could be argued that participant samples were specific to the male population most at risk of developing TC, namely well-educated males between the ages of 15 and 45 (Moore and Topping, 1999). Furthermore, these studies are not without their methodological shortcomings. Firstly, the method of data collection chosen by Goldenring and Purtell (1984) leaves a number of critical questions unanswered; only those participants responding correctly to the question 'What is the most common form of testicular cancer in a young male your age?' were asked where they had obtained their knowledge. It would perhaps have been beneficial to learn how misinformed participants had formed their views. Moreover, results of these studies lend themselves to demand characteristics, response set and social desirability biases due to the fact that self-reporting scales and instruments (including multiple-choice surveys) were used to measure knowledge of TC and practice of TSE. Moore and Topping (1999) report that 74% of participants correctly indicated that lumps were associated with TC, while 53% of male students in the Swedish sample expressed similar views. This could lead to erroneous assumptions being made regarding the level of TC knowledge held amongst these male samples; lumps are associated with cancers in general and it could well be argued that participants were simply attempting to guess the correct answer (Moore and Topping, 1999).
Interestingly, none of the studies cited above address the question of how masculine behaviours, norms and values might inform the ways in which young males understand TC and their TSE practices. From a social constructionist perspective, gender is practiced in social interactions and is signified by beliefs and behaviours; many men are socialised into believing that they are 'strong', and by reporting emotional and physical symptoms or discomfort they display signs of weakness (Moynihan, 1998). Should men ascribe to these socially constructed gender roles, both information-seeking and health-promoting behaviours may be inhibited (Lantz et al., 2001). This general reluctance to discuss personal concerns or health issues may extend into the doctor-patient relationship; men are often less forthcoming when seeking medical attention and less likely to provide specific details regarding their health concerns (Kroenke and Spitzer, 1998). Moreover, while females often rely on their GP for sources of healthcare information, males are more likely to use family, friends and electronic media as sources of information (Meissner et al., 1992). Men who take this passive role when seeking healthcare information are often less informed about health and the screening options available (Meissner et al., 1992).
For Wynd (2002), social support is a factor of increasing interest in helping young men to understand the importance of periodic TSE, and the need to seek medical attention should symptoms ever be detected. Research indicates that a lack of social support differentiates those who rarely (or never) practise TSE from those who perform TSE on a monthly basis (Wynd, 2002). In examining the applicability of the theory of reasoned action (TRA) (Ajzen and Madden, 1986) in relation to TSE performance, Brubaker and Wickersham (1990) reported that subjective norms may in fact enhance a man's intention to perform TSE. However, Finney, Weist and Friman (1995) subsequently examined the efficacy of social support as a means of TSE adherence. On this occasion, social support was found to have no effect on TSE adherence, or frequency of performance (Finney et al., 1995). Nevertheless, the intention to practice TSE is considered by many to be a key component in men's testicular health practices (Lechner et al., 2002; McGilligan et al., 2009). While the provision of healthcare information can increase men's intentions to practice TSE, attitudinal factors have been shown to mediate the relationship between knowledge and TSE practice (Lechner et al., 2002). Summarising past research, Poljski et al. (2003) identify a number of attitudinal barriers to performing TSE and include: perceptions of being immune to TC; the belief that TSE is not important to health; perceived embarrassment or difficulty in performing TSE; expectations of TSE becoming an awkward (or time-consuming) process; concerns about the reliability of TSE; and fears about what TSE may reveal.
Given that health professionals and cancer registries recommend monthly TSE, and the fact that few researchers have previously assessed male knowledge and awareness of TC, the next step would be to determine the current level of TC knowledge amongst young adult males using qualitative forms of data collection. A comprehensive review of the literature revealed that past research has relied heavily on direct measures, namely self-reporting scales and instruments including multiple-choice surveys and health-risk appraisals; methods which, on the whole, lend themselves to demand characteristics, response set and social desirability biases. Additionally, while direct measures are both economical and quick to employ, they are ultimately concerned with the strength of attitudes as opposed to the content or essence of attitudes. Using Q-methodology, this study sought to address gaps in the literature through exploring the diverse range of accounts that young males construct in relation to TC. Q-methodology was devised by British physicist William Stephenson in the 1930s, and provides a means of exploring subjective structures, attitudes and perspectives in a range of situations, from the standpoint of the person's lived experience (Brown, 1996; Cross, 2005b). The methodology is reported to have evolved from factor analytic theory (Brown, 1997). Essentially, Q-methodology allows many 'voices' to be heard (Stainton Rogers, 1995), and focuses on the range and diversity of views being expressed rather than the percentage of people expressing them (Kitzinger, 1987). The aim of Q-methodology is not to seek the truth, but to collect and explore the variety of accounts that people construct around a particular topic (Kitzinger, 1987; Cross, 2005a).
Method
Participants
Following ethical approval from Teesside University's ethics committee, seven male participants assisted with the piloting phase of the research, from an opportunity sample of psychology undergraduates studying at Teesside University. The final sample consisted of 27 males between the ages of 18 and 43 (mean age = 23.41, SD = 6.02). Twenty-three participants (85.2%) were recruited from psychology courses at Teesside University; most of whom responded to an advertisement placed on the University's managed research participation system. Additionally, four participants (14.8%) known to the researcher were recruited for the study via E-mail and in person. All participants were recruited for the study on a voluntary basis. In terms of demographics, 24 participants (88.9%) identified their ethnic background as being white British/Caucasian, one (3.7%) as black/black British, one (3.7%) as mixed race, and one (3.7%) as Chinese/Asian. Nineteen participants (70.4%) identified themselves as being single, while the remaining eight participants (29.6%) stated they were married or cohabiting.
Development of the Q-set
Q-set statements were derived from academic literature and published research, health promotion literature, practical guides, attitude instruments developed during past research, and through what is 'sayable' about TC more generally. The guiding principle in selecting the statements for the Q-set was to aim for a diverse representation of ideas, opinions and discourses on the subject, to allow participants to engage with a varied range of viewpoints.
Pilot phase
A pilot study was initially employed as a means of refining and/or adjusting the Q-set in order to minimise replication, and to ensure the representativeness of the final selection of statements. Seven male participants were provided with a master list containing an initial pool of 83 statements; participants were asked to identify which statements they agreed or disagreed with, and to identify statements for which they generally held no opinion. Additionally, pilot participants were instructed to provide general feedback on the initial pool of items should they find certain statements or terminology confusing. Duplicates and ambiguities were removed, and statements were generally discarded if pilot participants found them difficult to understand. Statements which yielded 'no opinion' were subsequently removed from the Q-set, as were any statements for which participants demonstrated complete agreement (or disagreement). This particular method of pilot testing is consistent with previous research adopting Q-methodology (Wright et al. 2007). Based on piloting results and participant feedback, 45 statements were selected for inclusion in the final Q-set (Appendix A).
Materials
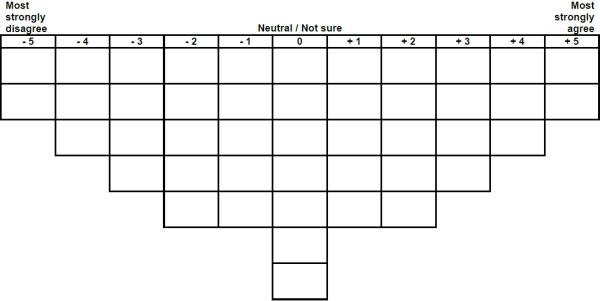
Participants were provided with detailed instructions, 45 randomly numbered statement cards and Q-sort response grid (Appendix B), demographic questionnaire, and an additional comments booklet (which included the open-ended question 'Where do you feel your attitudes towards testicular cancer have come from?'). The Q-sort response grid matrix contained spaces for 45 statements in columns below a scale with integers ranging from -5 (most strongly disagree) through to +5 (most strongly agree).
Procedure
Participants were instructed to familiarise themselves with each of the 45 Q-set statements, and to arrange the cards into three piles according to the extent to which they agreed or disagreed with each statement. Participants were then requested to sort the 45 Q-set statement cards along a continuum from -5 (strongly disagree) through to +5 (strongly agree) according to the shape of the Q-sort response grid matrix (forced normal distribution). On completion of the Q-sorting task, participants were advised that they were free to make changes, prior to confirming their final arrangement.
Immediately following the Q-sorting task, participants were asked to elaborate on their sorting choices, by commenting on the statements they had most agreed or disagreed with. Additionally, participants were asked to comment on statements they had deemed confusing or particularly difficult to understand, and to provide an answer to the open-ended question. Finally, participants completed a short demographic questionnaire concerning age, marital status and ethnic origin. On completion of the study, all participants were thanked for their participation and provided with debrief documentation. It was felt that the study may potentially bring to light specific health concerns in relation to TC. Accordingly, participants were also provided with contact details for support organisations, namely Teesside University's counselling service and NHS Direct, on the basis that further advice may be sought.
Results
Statistical overview
The 27 completed Q-sorts were entered into the dedicated Q analysis programme PCQ (Stricklin and Almeida, 2010), and statistically analysed using centroid factor analysis and varimax rotation. Eight factors emerged from the analysis, which explained 59% of the total variance and accounted for 16 of the 27 participants. Nine of the remaining 11 participants significantly loaded upon two or more factors (designated as confounded). Only factors presenting an Eigenvalue greater than unity (EV> 1.00) together with two or more factor exemplars were interpreted. Factor loadings and the sorts determined to be defining for each factor are displayed in Table 1. Factor interpretation was based primarily on the positioning of statements in each factor, combined with the open-ended responses and comments of those participants loading significantly upon these factors. Each interpreted factor was given a descriptive title, and a summary of each factor is presented below in narrative form. In order to maintain anonymity, pseudonyms will be used when referring to individual participants.
| Factor loadings | ||||
|---|---|---|---|---|
| Sort | 1 | 2 | 3 | 4 |
| 1. | 43 | 28 | 40 | 18 |
| 2. | 10 | 63X | 25 | 12 |
| 3. | 22 | 50X | -7 | 21 |
| 4. | 57 | 15 | 12 | 44 |
| 5. | 51 | 15 | 29 | 39 |
| 6. | 13 | 6 | 1 | 60X |
| 7. | 31 | 27 | 7 | 13 |
| 8. | 17 | 12 | 17 | 24 |
| 9. | 0 | 18 | 30 | 3 |
| 10. | 17 | 28 | 65X | 3 |
| 11. | 11 | 13 | -4 | 11 |
| 12. | 32 | 19 | 28 | 35 |
| 13. | 29 | 61 | 9 | -15 |
| 14. | 66X | 9 | 13 | 3 |
| 15. | 20 | 34 | 19 | 46 |
| 16. | 4 | 8 | 3 | 11 |
| 17. | 26 | 24 | 27 | 9 |
| 18. | 25 | 31 | 28 | -7 |
| 19. | 12 | 63X | 21 | 28 |
| 20. | 8 | 41 | 33 | 57 |
| 21. | 58X | 30 | 35 | 6 |
| 22. | 0 | 62X | 14 | 11 |
| 23. | 18 | -8 | 57X | 22 |
| 24. | 19 | 28 | 7 | 14 |
| 25. | 13 | 22 | 26 | 5 |
| 26. | 31 | 53 | -3 | 18 |
| 27. | 2 | 20 | 19 | 47X |
| Defining sorts | 2 | 4 | 2 | 2 |
| % expl. Variance | 9 | 12 | 7 | 8 |
Table 1: Factor matrix with an X indicating a defining sort.
Factor interpretations
Factor 1: Media influenced
Factor 1 explains 9% of the study variance, and has an Eigenvalue of 2.41. Two participants loaded significantly onto factor 1, as did three other participants with confounding Q-sorts. The theoretical array and key statements can be found in table 2. The two participants who loaded significantly onto factor 1 demonstrate a positive view of health promotion, and they acknowledge the role that TSE plays in the early detection and treatment of TC. This was particularly evident in participant open-ended comments; both participants indicated that the media had influenced their attitude towards TC. Anthony (all names are pseudonyms) specifically stated that he had formed his views on the back of 'media adverts and warnings from the NHS', while Duncan commented that the 'Know Your Balls…Check 'Em Out!' campaign has been 'well advertised'. Participants who share this perspective acknowledge that TC is highly treatable, and recognise that the majority of testicular lumps, bumps and swellings are not cancerous. Consistent with this, participants endorsed statements concerning testicular changes, and they strongly disagreed with the notion that TC often results in poor quality of life. While participants asserted that the fear of being labelled a hypochondriac should not discourage men from consulting their doctor about any testicular changes, they reported only mild agreement (or disagreement) with statements concerning the psychological, psychosexual or emotional effects of cancer.
| 6 | ||||||||||
| 18 | ||||||||||
| 3 | 4 | 19 | 1 | 7 | ||||||
| 2 | 12 | 13 | 24 | 15 | 8 | 9 | ||||
| 5 | 10 | 21 | 14 | 30 | 17 | 16 | 20 | 25 | ||
| 11 | 27 | 35 | 38 | 23 | 31 | 34 | 22 | 33 | 26 | 41 |
| 29 | 28 | 37 | 40 | 45 | 44 | 43 | 36 | 39 | 32 | 42 |
| No. | Statement. | Array position |
|---|---|---|
| Nine highest ranked statements (mostly agree) | ||
| 41. | The 'Know Your Balls… Check 'Em Out!' campaign aims to promote awareness of testicular cancer and testicular self-examination. | +5 |
| 42. | Vasectomy does not increase the risk of a man developing testicular cancer. | +5 |
| 25. | With early diagnosis, testicular cancer can be successfully treated in 98% of cases. | +4 |
| 26. | Most men who have testicular discomfort do not have cancer. | +4 |
| 32. | Testicular cancer is highly treatable. | +4 |
| 9. | Testicular cancer is the highest risk cancer for men between the ages of 15 and 45. | +3 |
| 20. | Testicular self-examination reduces anxiety and encourages young men to take greater responsibility for their health. | +3 |
| 33. | Testicular cancer is responsible for approximately 2% of all male cancers. | +3 |
| 39. | Most lumps found on the testicles are benign. | +3 |
| Nine lowest ranked statements (mostly disagree) | ||
| 11. | If testicular cancer occurs in one testicle, it is likely to occur in the other. | -5 |
| 29. | The most straightforward and safest way of dealing with a cancerous lump is to remove the testicle. | -5 |
| 5. | Testicular cancer is often terminal and leads to poor quality of life. | -4 |
| 27. | Testicular cancer is associated with injury and sporting strains. | -4 |
| 28. | Keeping a mobile phone in your trouser pocket can trigger testicular cancer. | -4 |
| 2. | There are no warning signs associated with testicular cancer. | -3 |
| 10. | The majority of lumps and swellings found on the testicles are the result of testicular cancer. | -3 |
| 35. | The fear of being labelled a hypochondriac prevents young men from consulting their doctor. | -3 |
| 37. | Testicular cancer only affects older age groups (men over the age of 55). | -3 |
Table 2: Factor 1 (Media Influenced) theoretical array and key statements.
Factor 2: Knowledgeable
Factor 2 explains 12% of the variance, and has an Eigenvalue of 3.26. Factor 2 had four significantly loading participants, making this the strongest factor to emerge from the analysis. In addition, three participants with confounding Q-sorts loaded significantly on this factor. The theoretical array and key statements can be found in table 3. The four participants who exemplified factor 2 demonstrate having substantial prior knowledge of TC. Two participants commented that they had learnt about TC during school health presentations, while Bradley commented that 'having a father who had and was successfully treated for prostate cancer and a mother who died from pancreatic cancer makes one all the more aware of cancer, and early detection'. A key theme of this account is that TC is seen to be highly treatable, and participants recognise the potential benefits of early diagnosis and treatment. Consistent with this, participants who share this perspective demonstrate a positive view of public education and awareness campaigns promoting TC and TSE, and they do not feel that such campaigns are likely to increase anxiety amongst young males. Moreover, participants rejected the notion that masculine values might inform the ways in which young males think about TC. Although the participants who loaded onto factor 2 appear knowledgeable about the common symptoms associated with TC, they demonstrate a limited understanding of the potential risk factors for TC. However, participants were completely dismissive of non-factual statements and myths concerning the cause of TC.
| 15 | ||||||||||
| 18 | ||||||||||
| 8 | 5 | 19 | 11 | 16 | ||||||
| 1 | 9 | 10 | 21 | 14 | 26 | 7 | ||||
| 34 | 2 | 13 | 12 | 38 | 33 | 29 | 17 | 6 | ||
| 27 | 37 | 3 | 30 | 23 | 43 | 40 | 32 | 22 | 25 | 4 |
| 28 | 45 | 24 | 31 | 36 | 44 | 42 | 39 | 35 | 41 | 20 |
| No. | Statement. | Array position |
|---|---|---|
| Nine highest ranked statements (mostly agree) | ||
| 4. | Brothers or sons of men who have had testicular cancer have an increased risk of testicular cancer. | +5 |
| 20. | Testicular self-examination reduces anxiety and encourages young men to take greater responsibility for their health. | +5 |
| 6. | There are a number of different types of testicular cancer. | +4 |
| 25. | With early diagnosis, testicular cancer can be successfully treated in 98% of cases. | +4 |
| 41. | The 'Know Your Balls… Check 'Em Out!' campaign aims to promote awareness of testicular cancer and testicular self-examination. | +4 |
| 7. | Testicular cancer often results in an ache or heavy feeling in the groin. | +3 |
| 17. | The exact causes of testicular cancer are unknown. | +3 |
| 22. | School is the most appropriate place to be taught testicular self-examination. | +3 |
| 35. | The fear of being labelled a hypochondriac prevents young men from consulting their doctor. | +3 |
| Nine lowest ranked statements (mostly disagree) | ||
| 27. | Testicular cancer is associated with injury and sporting strains. | -5 |
| 28. | Keeping a mobile phone in your trouser pocket can trigger testicular cancer. | -5 |
| 34. | Testicular cancer results in a loss of masculinity. | -4 |
| 37. | Testicular cancer only affects older age groups (men over the age of 55). | -4 |
| 45. | Testicular cancer is associated with a rash on the scrotum. | -4 |
| 1. | Health campaigns promoting testicular self-examination only increase anxiety amongst young men. | -3 |
| 2. | There are no warning signs associated with testicular cancer. | -3 |
| 3. | Tight underpants can cause testicular cancer. | -3 |
| 24. | Testicular cancer is more common in men who have a testicle that has failed to descend. | -3 |
Table 3: Factor 2 (Knowledgeable) theoretical array and key statements.
Factor 3: Cautious
Factor 3 explains 7% of the study variance, and has an Eigenvalue of 1.95. Two participants loaded significantly onto factor 3, as did one other participant with a confounding Q-sort. The theoretical array and key statements can be found in table 4. The participants who loaded significantly onto factor 3 appear somewhat fearful of TC, and for one of the participants his views are based on the personal experience of losing a family member to TC. In response to the open-ended question, Damian provided the following comment:
My dad's uncle died from testicular cancer which has made me aware of the painful death he suffered, so I have strong views on looking after yourself and self-checking regularly - even at an early age.
Moreover, Damian kindly provided additional comments in relation to statement 40:
People do not want to believe they will get it because their dad will get it, so they choose not to get checked. There should be screening done as soon as you are 40 to prevent early onset of testicular cancer.
Taking the above comments into account, it would seem that the participants see TC as being a disease which affects men aged 40 years and above only. However, this view was not reflected in the positioning of certain statements within this specific factor (items 9 and 37). Nonetheless, the participants who share this view understand that TC is rare in comparison to other forms of cancer, and they acknowledge that successful treatment is heavily reliant upon early detection.
| 1 | ||||||||||
| 4 | ||||||||||
| 8 | 3 | 6 | 7 | 9 | ||||||
| 10 | 20 | 5 | 14 | 13 | 16 | 23 | ||||
| 2 | 15 | 21 | 12 | 18 | 19 | 33 | 25 | 32 | ||
| 11 | 34 | 17 | 24 | 29 | 38 | 30 | 39 | 26 | 40 | 22 |
| 27 | 37 | 31 | 44 | 45 | 42 | 36 | 43 | 28 | 41 | 35 |
| No. | Statement. | Array position |
|---|---|---|
| Nine highest ranked statements (mostly agree) | ||
| 22. | School is the most appropriate place to be taught testicular self-examination. | +5 |
| 35. | The fear of being labelled a hypochondriac prevents young men from consulting their doctor. | +5 |
| 32. | Testicular cancer is highly treatable. | +4 |
| 40. | Inherited genetic factors are important in testicular cancer. | +4 |
| 41. | The 'Know Your Balls… Check 'Em Out!' campaign aims to promote awareness of testicular cancer and testicular self-examination. | +4 |
| 23. | In over 25% of cases the cancer has already spread by the time of diagnosis. | +3 |
| 25. | With early diagnosis, testicular cancer can be successfully treated in 98% of cases. | +3 |
| 26. | Most men who have testicular discomfort do not have cancer. | +3 |
| 28. | Keeping a mobile phone in your trouser pocket can trigger testicular cancer. | +3 |
| Nine lowest ranked statements (mostly disagree) | ||
| 11. | If testicular cancer occurs in one testicle, it is likely to occur in the other. | -5 |
| 27. | Testicular cancer is associated with injury and sporting strains. | -5 |
| 2. | There are no warning signs associated with testicular cancer. | -4 |
| 34. | Testicular cancer results in a loss of masculinity. | -4 |
| 37. | Testicular cancer only affects older age groups (men over the age of 55). | -4 |
| 10. | The majority of lumps and swellings found on the testicles are the result of testicular cancer. | -3 |
| 15. | Testicular cancer is not routinely screened for in sexual health clinics. | -3 |
| 17. | The exact causes of testicular cancer are unknown. | -3 |
| 31. | More men die of testicular cancer than women do of breast cancer. | -3 |
Table 4: Factor 3 (Cautious) theoretical array and key statements.
Factor 4: Mislead
Factor 4 explains 8% of the variance, and has an Eigenvalue of 2.08. Two participants loaded significantly onto factor 4, as did four other participants with confounding Q-sorts. The theoretical array and key statements can be found in table 5. The participants who exemplified factor 4 would appear to be somewhat misguided about the subject of TC, with participants indicating that they had formed their views as a result of conversations with parents and peers. This was most certainly evident in the open-ended comments of both participants. In response to the open-ended question, Jake provided the following comment:
Mostly from a little information handed out over the years, as well as rumours and word of mouth etc. I think it does cause a lot of anxiety to men because the majority do not have all the information about it.
In addition, Patrick commented that he had previously been 'taught to look after himself' by his parents and teachers. These comments would indicate that there is a potential for young males to be provided with inaccurate healthcare information through informal conversation with family members, friends and school teachers. Accordingly, this account is characterised by conflicting views and an acceptance of inaccurate or misleading information concerning the risk factors and potential symptoms involved in TC. Although participants were dismissive of particular myths and non-factual statements, notably those concerning rashes on the scrotum and sporting strains and/or injuries, they believe there to be an association between tight underpants and increased cancer risk. In spite of these contradictory findings, participants acknowledge that young males are those most at risk of TC, and they recognise that TC is highly treatable in cases where the cancer is detected during the early stages.
| 6 | ||||||||||
| 14 | ||||||||||
| 10 | 4 | 22 | 1 | 3 | ||||||
| 2 | 12 | 7 | 34 | 5 | 18 | 11 | ||||
| 33 | 8 | 13 | 16 | 40 | 29 | 19 | 15 | 20 | ||
| 37 | 39 | 21 | 28 | 23 | 42 | 36 | 24 | 17 | 25 | 9 |
| 38 | 45 | 27 | 31 | 30 | 43 | 44 | 41 | 35 | 32 | 26 |
| No. | Statement. | Array position |
|---|---|---|
| Nine highest ranked statements (mostly agree) | ||
| 9. | Testicular cancer is the highest risk cancer for men between the ages of 15 and 45. | +5 |
| 26. | Most men who have testicular discomfort do not have cancer. | +5 |
| 20. | Testicular self-examination reduces anxiety and encourages young men to take greater responsibility for their health. | +4 |
| 25. | With early diagnosis, testicular cancer can be successfully treated in 98% of cases. | +4 |
| 32. | Testicular cancer is highly treatable. | +4 |
| 11. | If testicular cancer occurs in one testicle, it is likely to occur in the other. | +3 |
| 15. | Testicular cancer is not routinely screened for in sexual health clinics. | +3 |
| 17. | The exact causes of testicular cancer are unknown. | +3 |
| 35. | The fear of being labelled a hypochondriac prevents young men from consulting their doctor. | +3 |
| Nine lowest ranked statements (mostly disagree) | ||
| 37. | Testicular cancer only affects older age groups (men over the age of 55). | -5 |
| 38. | Testicular cancer is relatively rare compared to cancers such as lung or breast cancer. | -5 |
| 33. | Testicular cancer is responsible for approximately 2% of all male cancers. | -4 |
| 39. | Most lumps found on the testicles are benign. | -4 |
| 45. | Testicular cancer is associated with a rash on the scrotum. | -4 |
| 2. | There are no warning signs associated with testicular cancer. | -3 |
| 8. | Testicular cancer often results in hair loss. | -3 |
| 21. | Leukaemia is more common than testicular cancer in young men. | -3 |
| 27. | Testicular cancer is associated with injury and sporting strains. | -3 |
Table 5: Factor 4 (Mislead) theoretical array and key statements.
Discussion
As far as it is known, this is the first UK study to investigate TC knowledge and awareness amongst males aged 18 to 45 using Q-methodology. In doing so, this research has highlighted the potential of Q-methodology in exploring the diverse range of meanings or understandings that young adult males construct in relation to TC, and the need to explore this diversity as opposed to treating young males as a homogenous group. Participants' Q-sort responses represented four distinct perspectives concerning TC. These four perspectives were subsequently interpreted and given appropriate descriptive titles, namely Media Influenced, Knowledgeable, Cautious and Mislead.
With the exception of factor 4 (Mislead) consensus existed regarding the prevalence of TC amongst high risk male populations. This was illustrated by the positioning of statements across factors 1 (Media Influenced), 2 (Knowledgeable) and 3 (Cautious). Participants exemplifying factors 1 through to 3 demonstrated agreement with statements concerning TC incidence rates and statistics, albeit mildly. Equally notable were the contrasting views in relation to statements 21, 31 and 38. While factors 2 and 3 see TC as being a relatively rare form of cancer, factors 1 and 4 consider TC to be more common than lung and/or breast cancer. Although participants knew that TC most commonly affects males aged 15 to 45, there was general disagreement concerning the many causes and risk factors involved in TC.
Multiple statements addressed the genetic, biological and ethnic risk factors involved in TC. While different views were expressed between factors on this issue, exemplars tended to be very consistent in their response: they either did or did not agree that familial history, race and cryptorchidism increases TC risk. Responses to these particular statements were surprising, given that some exemplary participants indicated that they had previously lost family members to TC and other forms of cancer. One might expect participants with familial history of cancer to have a heightened awareness of the potential genetic and biological risk factors involved in TC; however this did not prove to be the case. With the exception of factors 3 and 4, participants were completely dismissive of non-factual statements and myths concerning the causes of TC. Interestingly, factor 4 exemplars asserted that tight underpants may increase TC risk, despite rejecting all notions of physical trauma and mobile phone usage having an adverse effect on TC risk.
Irrespective of specific factor loadings, participants were unanimous in acknowledging the role that TSE in plays in early detection and treatment of TC, while all participants agreed that TC is highly treatable. Nonetheless, there were contrasting views concerning the specific symptoms often associated with TC. Participants loading significantly onto factors 1, 2 and 3 were able to differentiate between the common symptoms of TC and the potential side effects of high-dose chemotherapy and radiotherapy; however factor 4 exemplars were not able to make the same distinction. Similarly, while participants exemplifying factors 1, 2 and 3 recognised that testicular lumps and areas of swelling are not always indicative of cancer, the same could not be said for factor 4 exemplars.
The findings reported above do not confirm past reports that young educated males lack knowledge of TC and do not recognise the importance of TSE. Although the sample is not directly comparable to those used in past studies, results of the present research indicate that males in the highest risk age group were more likely to have heard of TC and TSE than in previous studies assessing TC knowledge amongst males in academic populations. On the whole, participants exemplifying factors 1, 2 and 3 were informed about the causes and symptoms of TC, and understood the importance of periodic TSE. Perhaps most importantly, the present research provides evidence to suggest that increased media coverage of TC has led to increased levels of knowledge about the disease and the importance of self-screening. These results point towards an increase in awareness and practice of TSE over the last 10 years, or indeed may reflect the well-educated bias of the male participants in this research. One could reasonably expect psychology undergraduates to have a greater appreciation of health matters than peers in other disciplines, or indeed the wider population. Nonetheless, the improved level of TC knowledge and awareness shown by young adult males in comparison to past research is particularly gratifying.
The negative effects of socially constructed views of gender and masculinity on men's information-seeking and health-promoting behaviours are well documented (Moynihan, 1998; Lantz et al., 2001). As discussed earlier, adherence to these traditional masculine values often influence men's overall attitude towards healthcare, their preparedness to practice TSE, their willingness to seek cancer screening, and the ways in which they might seek help should they ever be diagnosed with TC. While results of the present research do not appear to support the current research position concerning the negative influence of masculine values on men's health-seeking behaviours, factors 2 (Knowledgeable), 3 (Cautious) and 4 (Mislead) may be interpreted using components of the TRA (Ajzen and Madden, 1986).
Of particular interest is the existence of a possible negative correlation between social support and TC knowledge in young adult males. Although factor 4 exemplars demonstrated some basic knowledge of TC, they were ultimately misguided about the causes and symptoms of TC. Perhaps more importantly, factor 4 exemplars indicated that they had formed their views through informal conversation with parents, peers and teachers. These findings may have important implications for the formulation of strategies aimed at improving young men's knowledge and awareness of TC and their adherence to self-screening practices. Recent recommendations put forward by healthcare professionals for improving TC awareness and encouraging TSE practice include the provision of dedicated health information websites and enhancements to doctor-patient relationships, together with an increase in the number of screening clinics at sports clubs and gymnasiums (Hall, 2003). Additionally, it has been suggested that females should be encouraged to promote health-seeking and related self-screening behaviours in their male partners (Norcross et al., 1996). In any case, young adult males should be reached through channels other than the medical arena, since they consult their GP (and other healthcare providers) less often than females, or indeed older males (de Nooijer et al., 2002).
The Q-set was limited by the omission of statements relating to the TSE procedure, or indeed how to perform TSE correctly or efficiently. Additionally, only four of the 45 statements explicitly mentioned TSE (items 1, 20, 22 and 41). As a result, this may have limited the opportunity for young males to express their understanding of TSE, or self-screening practices more generally.
Four distinct perspectives were identified during the course of this Q-methodological research. Still, it is important to note that these may not be the only ways in which young adult males construct meanings or understandings about TC. If the research was to be carried out again using alternative statements, different participants, or perhaps at a different point in time, it is likely that new perspectives may emerge from any analysis. While Q-methodology focuses on distinct perspectives as opposed to the overlap between perspectives, those males holding mixed (confounding) perspectives accounted for 33.3% of participants in the sample. Consequently, it would have been of some interest to learn how these participants construct their meanings and understandings of TC.
Although participant samples in Q-methodological research do not necessarily need to be representative, efforts should be made to ensure breadth and diversity so that a greater number of standpoints, meanings and understandings may be accessed (Darwin and Campbell, 2009). A diverse group of young males loaded both significantly and exclusively upon each of the four factors. Nonetheless, male participants from diverse ethnic backgrounds were mostly under-represented in this research; including males of varied socioeconomic or educational backgrounds, sexual orientations and/or gender identities might also have provided a more complete picture. Moreover, while the sample size is not inconsistent with other studies employing Q-methodology, a larger sample size might have enabled the findings to be developed further by providing additional insight about the degree to which participant's constructions of TC varied.
TC is the most common malignancy in males between the ages of 15 and 45, and predominantly strikes during the prime of life, at a time when important personal, career and family decisions are made. Cancer registries and support groups in the UK recommend that young men should be provided with, at minimum, a basic awareness of TC, and the knowledge that medical advice should be sought in the event that testicular lumps or masses are found. Overall, results of this Q-methodological study indicate that males in the highest risk age group for TC were more likely to have heard of TC and TSE, in comparison to past research assessing knowledge of the disease and self-screening practices. Nonetheless, some participants were ultimately misguided about the causes and symptoms of TC. Clearly, there is a need for continued research to understand the many factors influencing men's knowledge and awareness of TC, particularly with regards to social support, and to formulate strategies or interventions that will promote practice of TSE in young adult males.
Acknowledgments
This research was completed as an undergraduate dissertation in the School of Social Science and Law at Teesside University. I gratefully acknowledge the following people, without whom this research would not have been possible.
Sincere thanks go to my supervisor, Dr Glynis Gardiner, for providing invaluable feedback, support and guidance throughout the course of the research.
I extend my gratitude to the 27 males who participated in this research, along with the seven males who assisted during the piloting phase of the study. I would like to thank each and every one for their time and willingness to contribute to the research.
Finally, I would like to thank my parents and my partner, Angela Cummins, for their continuous and unconditional support throughout the course of my undergraduate studies.
Appendix A
| Q-set statements | |
|---|---|
| 1. | Health campaigns promoting testicular self-examination only increase anxiety amongst young men. |
| 2. | There are no warning signs associated with testicular cancer. |
| 3. | Tight underpants can cause testicular cancer. |
| 4. | Brothers or sons of men who have had testicular cancer have an increased risk of testicular cancer. |
| 5. | Testicular cancer is often terminal and leads to poor quality of life. |
| 6. | There are a number of different types of testicular cancer. |
| 7. | Testicular cancer often results in an ache or heavy feeling in the groin. |
| 8. | Testicular cancer often results in hair loss. |
| 9. | Testicular cancer is the highest risk cancer for men between the ages of 15 and 45. |
| 10. | The majority of lumps and swellings found on the testicles are the result of testicular cancer. |
| 11. | If testicular cancer occurs in one testicle, it is likely to occur in the other. |
| 12. | Testicular cancer is more common in white men than African-Caribbean or Asian men. |
| 13. | Men with fertility problems have an increased risk of testicular cancer. |
| 14. | Testicular cancer adversely affects sexual performance. |
| 15. | Testicular cancer is not routinely screened for in sexual health clinics. |
| 16. | Each year around 2,000 young men in the UK are diagnosed with testicular cancer. |
| 17. | The exact causes of testicular cancer are unknown. |
| 18. | Testicular cancer leads to feelings of being overwhelmed. |
| 19. | The majority of men with testicular cancer who undergo chemotherapy treatment become infertile. |
| 20. | Testicular self-examination reduces anxiety and encourages young men to take greater responsibility for their health. |
| 21. | Leukaemia is more common than testicular cancer in young men. |
| 22. | School is the most appropriate place to be taught testicular self-examination. |
| 23. | In over 25% of cases the cancer has already spread by the time of diagnosis. |
| 24. | Testicular cancer is more common in men who have a testicle that has failed to descend. |
| 25. | With early diagnosis, testicular cancer can be successfully treated in 98% of cases. |
| 26. | Most men who have testicular discomfort do not have cancer. |
| 27. | Testicular cancer is associated with injury and sporting strains. |
| 28. | Keeping a mobile phone in your trouser pocket can trigger testicular cancer. |
| 29. | The most straightforward and safest way of dealing with a cancerous lump is to remove the testicle. |
| 30. | Testicular cancer leads to weight loss. |
| 31. | More men die of testicular cancer than women do of breast cancer. |
| 32. | Testicular cancer is highly treatable. |
| 33. | Testicular cancer is responsible for approximately 2% of all male cancers. |
| 34. | Testicular cancer results in a loss of masculinity. |
| 35. | The fear of being labelled a hypochondriac prevents young men from consulting their doctor. |
| 36. | Blood in the urine is a common symptom of testicular cancer. |
| 37. | Testicular cancer only affects older age groups (men over the age of 55). |
| 38. | Testicular cancer is relatively rare compared to cancers such as lung or breast cancer. |
| 39. | Most lumps found on the testicles are benign. |
| 40. | Inherited genetic factors are important in testicular cancer. |
| 41. | The 'Know Your Balls… Check 'Em Out!' campaign aims to promote awareness of testicular cancer and testicular self-examination. |
| 42. | Vasectomy does not increase the risk of a man developing testicular cancer. |
| 43. | Testicular cancer leads to feelings of isolation. |
| 44. | Testicular cancer often results in unbearable pain. |
| 45. | Testicular cancer is associated with a rash on the scrotum. |
Appendix B
Q-sort response grid
Notes
[1] Ian completed his BSc in 2011 obtaining a First Class Honours Degree in Forensic Psychology at Teesside University, for which he received the British Psychological Society Undergraduate Award for the highest overall grade upon graduation in the 2010/11 academic year. Ian is currently undertaking the Professional Graduate Certificate in Education (Lifelong Learning Sector) at the University of Huddersfield.
References
Ajzen, I. and T. J. Madden (1986), 'Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control', Journal of Experimental Social Psychology, 22 (5), 454-74, DOI:10.1016/0022-1031(86)90045-4, accessed 1 April 2011
Boyle, P., S. B. Kaye and A. G. Robertson (1987), 'Changes in testicular cancer in Scotland', European Journal of Cancer and Clinical Oncology, 23 (6), 827-30, DOI: 10.1016/0277-5379(87)90286-0, accessed 16 March 2011
Bray, F., L. Richiardi, A. Ekbom, E. Pukkala, M. Cuninkova and H. Møller (2006), 'Trends in testicular cancer incidence and mortality in 22 European countries: Continuing increases in incidence and declines in mortality', International Journal of Cancer, 118 (12), 3099-111, DOI: 10.1002/ijc.21747, accessed 15 March 2011
Brown, S. R. (1996), 'Q-methodology and qualitative research', Qualitative Health Research, 6 (4), 561-567, http://www.lrz.de/~schmolck/qmethod/srbqhc.htm, accessed 25 September 2011
Brown, S. R. (1997), The History and Principles of Q-methodology in Psychology and the Social Sciences, http://facstaff.uww.edu/cottlec/Qarchive/Bps.htm, accessed 25 September 2011
Brubaker, R. G. and D. Wickersham (1990), 'Encouraging the practice of testicular self-examination: A field application of the theory of reasoned action', Health Psychology, 9 (2), 154-63, DOI: 10.1037/0278-6133.9.2.154, accessed 22 March 2011
Cancer Research UK (2010), Testicular cancer, http://www.cancerhelp.org.uk/type/testicular-cancer/, accessed 14 March 2011
Cross, R. M. (2005a), 'Accident and Emergency nurses' attitudes towards health promotion', Journal of Advanced Nursing, 51 (5), 474-483, DOI: 10.1111/j.1365-2648.2005.03517.x, accessed January 15, 2011
Cross, R. M. (2005b), 'Exploring attitudes: The case for Q methodology', Health Education Research, 20 (2), 206-13, DOI: 10.1093/her/cyg121, accessed 24 March 2011
Darwin, Z. and C. Campbell (2009), 'Understandings of cervical screening in sexual minority women: A Q-methodological study', Feminism & Psychology, 19 (4), 534-54, DOI: 10.1177/0959353509342919, accessed 15 January 2011
de Nooijer, J., L. Lechner and H. de Vries (2002), 'Early detection of cancer: Knowledge and behavior among Dutch adults', Cancer Detection and Prevention, 26 (5), 362-69, DOI: 10.1016/S0361-090X(02)00121-6, accessed 20 March 2011
Evans, R. E. C., A. Steptoe and J. Wardle (2006), ' Testicular self-examination: change in rates of practice in European university students, from 13 countries, over a 10-year period', The Journal of Men's Health & Gender, 3 (4), 368-72, DOI: 10.1016/j.jmhg.2006.08.005, accessed 14 March 2011
Everyman (no date), Testicular cancer, http://www.everyman-campaign.org/Testicular_Cancer/index.shtml, accessed 14 March 2011
Finney, J. W., M. D. Weist and P. C. Friman (1995), ' Evaluation of two health education strategies for testicular self-examination', Journal of Applied Behavior Analysis, 28 (1), 39-46, DOI: 10.1901/jaba.1995.28-39, accessed 22 March 2011
Gascoigne, P., M. D. Mason and E. Roberts (1999), 'Factors affecting presentation and delay in patients with testicular cancer: Results of a qualitative study', Psycho-Oncology, 8 (2), 144-54
Goldenring, J. M. and E. Purtell (1984), 'Knowledge of testicular cancer risk and need for self-examination in college students: A call for equal time for men in teaching of early cancer detection techniques', Pediatrics, 74 (6), 1093-96
Güleser, G. N. and D. Unalan (2010), 'The knowledge, attitude and behaviours of healthy services vocational students on testicular cancer and testicular self-examination', European Journal of Oncology Nursing, 14 (S1), S35
Hall, R. H. (2003), 'Promoting men's health', Australian Family Physician, 32 (6), 401-07, http://www.racgp.org.au/afp/200306/20030601hall.pdf, accessed 31 March 2011
Handy, P. and K. N. Sankar (2008), 'Testicular self examination: Knowledge of men attending a large Genito Urinary Medicine clinic', Health Education Journal, 67 (1), 9-15, DOI: 10.1177/0017896907083152, accessed 20 March 2011
Kitzinger, C. (1987), The Social Construction of Lesbianism, Bristol: Sage Publications
Kroenke, K. and R. L. Spitzer (1998), 'Gender differences in the reporting of physical and somatoform symptoms', Psychosomatic Medicine, 60 (2), 150-55
Lantz, J. M., J. T. Fullerton, R. J. Harshburger and G. Robins Sadler (2001), 'Promoting screening and early detection of cancer in men', Nursing and Health Sciences, 3 (4), 189-96, DOI: 10.1046/j.1442-2018.2001.00088.x, accessed 21 March 2011
Lechner, L., A. Oenema and J. de Nooijer (2002), ' Testicular self-examination (TSE) among Dutch young men aged 15-19: Determinants of the intention to practice TSE', Health Education Research, 17 (1), 73-84
McGilligan, C., C. McClenahan and G. Adamson (2009), ' Attitudes and intentions to performing testicular self-examination: Utilizing an extended theory of planned behavior', Journal of Adolescent Health, 44 (4), 404-06, DOI: 10.1016/j.jadohealth.2008.08.018, accessed 23 March 2011
Meissner, H. I., A. L. Potosky and R. Convissor (1992), ' How sources of health information relate to knowledge and use of cancer screening exams', Journal of Community Health, 17 (3), 153-65
Moore, R. A. and A. Topping (1999), 'Young men's knowledge of testicular cancer and testicular self-examination: A lost opportunity?', European Journal of Cancer Care, 8 (3), 137-42, DOI: 10.1046/j.1365-2354.1999.00151.x, accessed 14 March 2011
Moynihan, C. (1998), 'Theories in health care and research: Theories of masculinity', British Medical Journal, 317 (7165), 1072-075
NHS Choices (2010), Testicular cancer, http://www.nhs.uk/conditions/cancer-of-the-testicle/Pages/Introduction.aspx, accessed 14 March 2011
Norcross, W. A., C. Ramirez and L. A. Palinkas (1996), ' The influence of women on the health care-seeking behavior of men', The Journal of Family Practice, 43 (5), 475-80
Poljski, C., C. Andrews, C. Holden and D. de Kretser (2003), 'Needs analysis of community education in Australia on testicular cancer', Andrology Australia, 1(Suppl. 3), http://www.andrologyaustralia.org/UserFiles/File/x03_TesticularCancer_Suppl3.pdf, accessed 21 March 2011
Richie, J. P. (1993), 'Detection and treatment of testicular cancer', A Cancer Journal for Clinicians, 43 (3), 151-75, DOI: 10.3322/canjclin.43.3.151, accessed 16 March 2011
Rudberg, L., S. Nilsson, K. Wikblad and M. Carlsson (2005), 'Testicular cancer and testicular self-examination: Knowledge and attitudes of adolescent Swedish men', Cancer Nursing, 28 (4), 256-62
Stainton Rogers, R. (1995), 'Q-methodology' in Smith, J.A., Harre, R. and Van Langenhove, L. (eds.), Rethinking Methods in Psychology, London: Sage Publications, pp. 178-192
Stricklin, M. and J. Almeida (2010), PCQ for Windows: Analysis software for Q-technique [Computer program]
Ugurlu, Z., G. Akkuzu, A. Karahan, A. Beder, N. Dogan, S. Okdem and S. Kav (2010), 'Testicular cancer and testicular self-examination knowledge and practice among university students', European Journal of Oncology Nursing, 14 (S1), S36
Wright, D. W., L. A. Simmons and K. Campbell (2007), 'Does a marriage ideal exist? Using Q-sort methodology to compare young adults' and professional educators' views on healthy marriages', Contemporary Family Therapy: An International Journal, 29 (4), 223-236, DOI: 10.1007/s10591-007-9044-0, accessed 21 January 2011
Wynd, C. A. (2002), 'Testicular self-examination in young adult men', Journal of Nursing Scholarship, 34 (3), 251-55, DOI: 10.1111/j.1547-5069.2002.00251.x, accessed 17 March 2011
To cite this paper please use the following details: Garner, I. (2011), 'Understandings of testicular cancer in young adult males: A Q-methodological study', Reinvention: a Journal of Undergraduate Research, Volume 4, Issue 2, http://ww.warwick.ac.uk/go/reinventionjournal/issues/volume4issue2/garner Date accessed [insert date]. If you cite this article or use it in any teaching or other related activities please let us know by e-mailing us at Reinventionjournal at warwick dot ac dot uk.