
Hand Hygiene Research
Research Area
I am interested in the complex challenge of ensuring healthcare professionals are able to perform hand hygiene to evidence-based standards, and their ability to receive meaningful, useful feedback on this performance. My work explores both manual and electronic routes to provide assistance within this field, with a clear emphasis on the need to involve healthcare professionals in the process of developing new systems of measurement. This can ensure processes and innovations are Fit For Purpose, and build upon existing behavioural patterns and predispositions.
The Role of Hand Hygiene in Infection Control
According to the World Health Organisation's (WHO, 2009) report1 hand hygiene is the key factor in the cross-contamination which can lead to occurrences of Healthcare Associated Infections (HCAI). Empirical evidence in favour of this conclusion has built up strongly over the past 40 years.2-7 To graphically illustrate how cross-contamination can occur through hand contact, and therefore poor hand hygiene, WHO (2009) published a series of figures (see below) which show (i) how hands can become contaminated, (ii) how inadequate hand hygiene can fail to remove contamination (ii) how such contamination can be spread. This spreading can be within the Patient-healthcare professional relationship, the Patient Zone (the area and environment immediately surrounding the individual Patient) and also between Patients through healthcare professional contact.
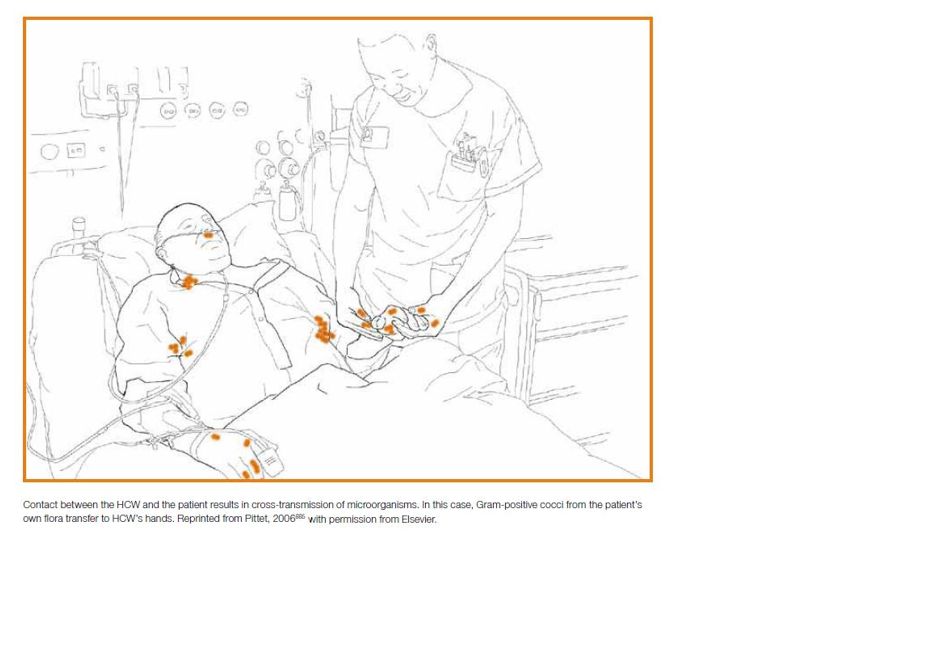

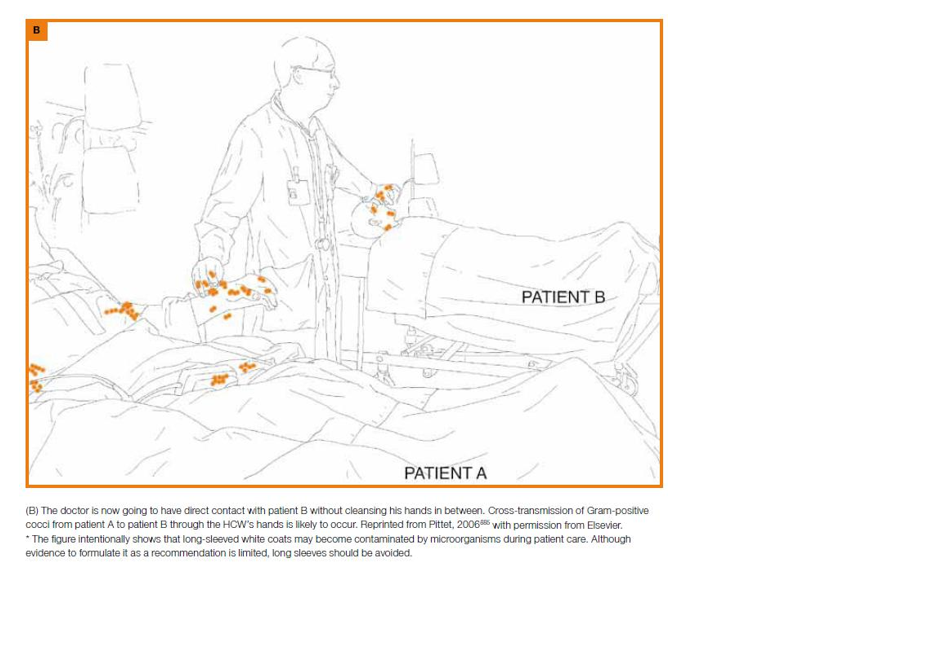
These figures can also be seen in context at Pages 15-21 of the WHO 2009 Report1. Please note that all corresponding text alongside the figures are part of the original works.
The WHO 5 Moments
A key development in the ongoing "battle" to improve knowledge about the importance of hand hygiene has been the development of the "My 5 Moments for Hand Hygiene" (see below).
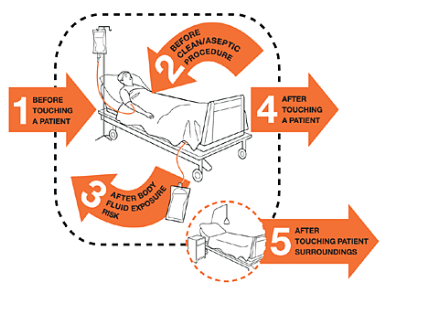
These promotional guidelines were developed by the World Health Organisation8, as part of their Clean Care is Safer Care initiative9. Launched in 2007 with an aim to be a tool that "bridges the gap between scientific evidence and daily health practice"8, the specific 5 Moments (see above) indicate when hand hygiene should be performed when within the Patient Zone, the area around an individual Patient including their immediate surroundings, belongings and environment. This Patient Zone is represented in the figure (above) by the "dotted line", therefore the Patient Zone includes both equipment (Patient bed and IV Stand), as well as the Patient themselves. Any bedside cabinet, chair or table present would also be part of this Patient Zone.
Obtaining Hand Hygiene Compliance: A Continuing Challenge
Despite empirical evidence of the role of hand hygiene in reducing cross-contamination, and global guidelines generated by the collaboration of world leaders within the field, it is acknowledged that obtaining compliance to required hand hygiene standards remains a challenge.1,9 A summary of the wealth of research carried out on hand hygiene adherence over the past 35 years (1977 onwards), demonstrated the vast fluctuations between healthcare professional hand hygiene compliance rates: from 5% to 89%, with a resultant average of 38.7%1,10,11.
Measuring Hand Hygiene Compliance: Are Interventions Working?
The challenge obtaining compliance is compounded by problems accurately and efficiently measuring how well, or otherwise, healthcare professionals are adhering to given standards. A Cochrane review in 201012 concluded that whilst a multitude of different intervention styles were being applied to the area of hand hygiene, the quality and consistency of these varied greatly, with only 4 out of 129 studies meeting their inclusion criteria.
Prior to implementing strategies to improve hand hygiene compliance, first the current performance level must be established, to assess the impact of any intervention. A successful process needs to monitor hand
hygiene by detecting it has been required, and measure the details of the event to record whether decontamination occurred. It must also provide feedback to allow analysis and focus on subsequent priorities for performance change. Each of the main methods of measuring hand hygiene, namely self-reporting, indirect measurement and direct observation, have established strengths and weaknesses.13 It is direct observation, however, which is considered the "gold standard" approach.14-17
The Audit Process
Auditing, a standard measurement procedure from the Quality Management approach, has been widely adopted as a method of data collection within healthcare hand hygiene assessment.18 The aim of auditing is to provide a mechanism for the collection of data which can then be used to determine future resource needs, for example additional training. Hand hygiene auditing has seen the development of a number of tools, including those specifically designed to allow observation and measurement of performance at the WHO 5 Moments.19 However, even such tools which use methods of direct observation, deemed the gold standard by the WHO, only offer snap shots of hand hygiene. They may also provoke the highlighted Hawthorne effect.20 Manual auditing also poses limitation in terms of being resource intensive, often involving clinical staff being involved in the collection, analysis and feedback phases of the audit. Scope thus remains for alternative methods of measurement.
The Potential Role of Technology
Technology offers two potential roles within this field: (i) to reduce the burden of the audit process, (ii) to improve compliance to hand hygiene guidelines.
Technology has been trialled in other sectors to ensure compliance to essential cleanliness protocols, for example the food industry21 and the space industry22 (see below). Aims have been to reduce labour intensive aspects of ensuring compliance and addressing the potentially flawed method of direct observation.
Work has been undertaken within the area of healthcare professional hand hygiene.23-25 There has been a rise in electronic monitoring systems, and innovations promoted to provide auditing capacity. However, these are limited in their ability to capture all of the WHO 5 Moments.
There also appears to be a lack of evidence that the concept of domain knowledge has been considered, in order to ensure that the technology is Fit For Purpose. Involvement of proposed end users can result in perceptions of increased usefulness and perceived ease of use. Interestingly, these perceptions can be from those involved in an innovations’ development, and also those made aware that it was developed involving peers from their expert area (i.e. other healthcare professionals).26,27
Hand Hygiene and Human Behaviour
Behavioural research suggest that different instances of hand hygiene may be triggered in separate ways.28,29 Indeed, Whitby et al. (2006)28 postulate two forms of hand hygiene behaviour: Inherent and Elective.
Inherent hand hygiene is an instinctive need driven by themes of self-protection. It links to decontamination at times when the hands are visibly dirty, contaminated for example by blood, or after touching an emotionally dirty area such as a Patient's groin.
Elective hand hygiene relates to opportunities where instinctive hand hygiene does not occur. Perhaps when hands appear clean, or the area touched is not emotionally dirty (e.g. taking a pulse), yet decontamination is still required. Therefore hand hygiene has to be premeditated, it is not automatic.
Whitby et al. (2006, 2007)28,29 suggest that it is with Elective hand hygiene that opportunities are more likely to be missed. Therefore interventions may have more impact if they consider the type of activity (Inherent/Elective), and the predisposed likelihood of an individual to perform hand hygiene: where are prompts needed most?