
Pandemics and inequality
Pandemics and inequality
Thursday 3 Dec 2020Pandemics of the past have had major consequences for inequality, not all of them positive. What lessons can we learn about the potential redistributive effects of COVID-19? Guido Alfani explores the impact of plague and influenza on inequality, and asks how infection spread and mortality rates affect wealth and income redistribution.
The Black Death and subsequent plagues
The Black Death, which struck Europe and the Mediterranean during 1347–52 killing about half the population of the area, caused a significant and long-lasting reduction in wealth and income inequality. This is clearly visible in Italy (Fig.1), which is the area for which we currently have the best information. In the aftermath of the Black Death, the richest 10% of the population lost their grip on between 15 and 20% of their overall wealth, and pre-plague levels were not reached again before the second half of the seventeenth century.
Figure 1. The share of wealth of the top 10% in Italy, 1300–1800
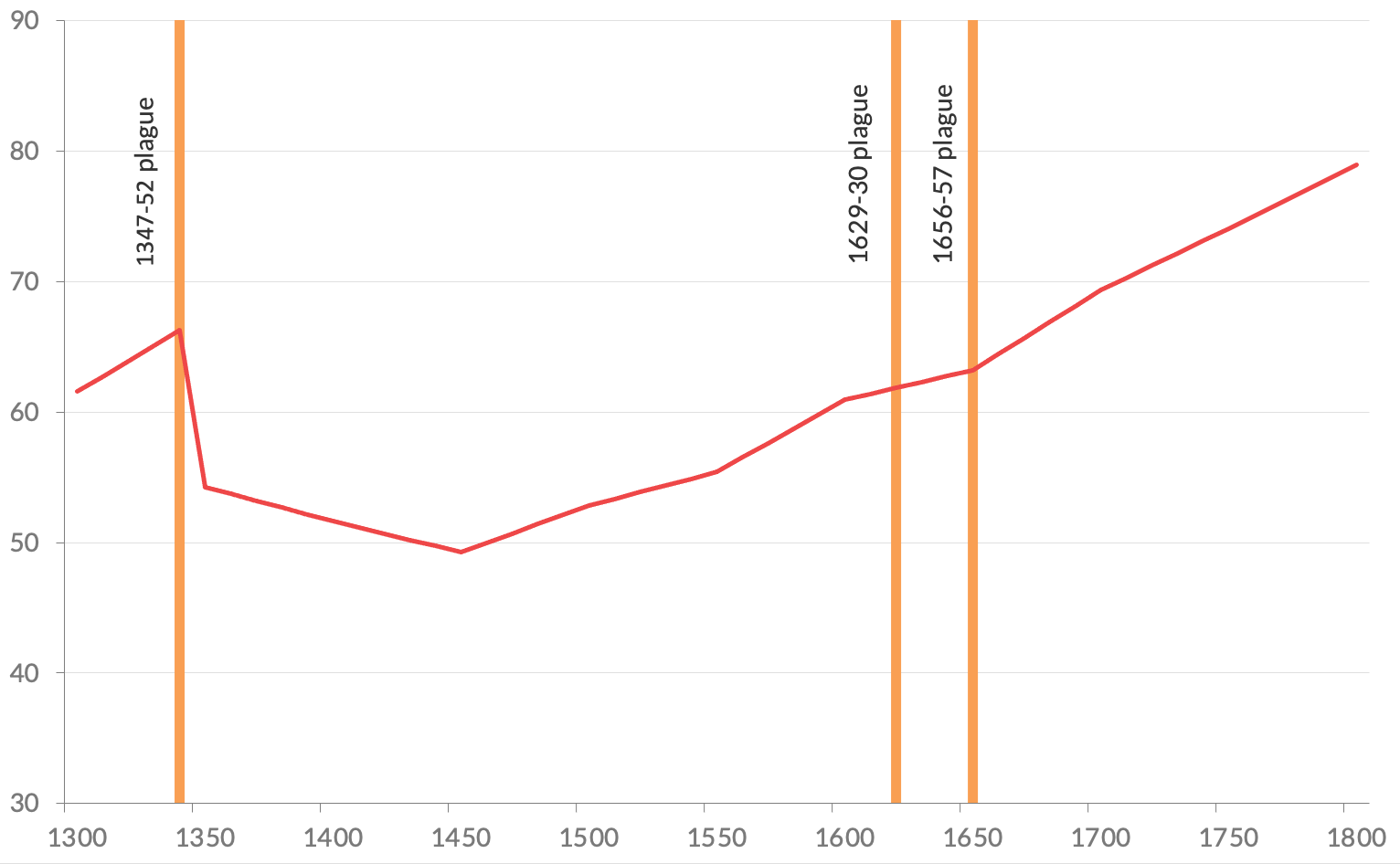
Source: elaboration based on Alfani, 2021
Based on the example of the Black Death, the view that pandemics had the power to (brutally) level inequality has become quite widespread among scholars and in civil society. However, if we take into account subsequent pandemics, it becomes apparent that the Black Death was exceptional, even if we compare pandemics caused by the same pathogen. In Italy, no reduction in wealth inequality can be observed after the seventeenth-century plagues (Fig.1). As elsewhere in south Europe, these were the worst plagues after the Black Death and were characterised by very high mortality rates: 35% in 1629–30 when plague spread to north Italy and Tuscany, and 40% in 1656–57 when it affected the central and southern regions (except for Tuscany) (Alfani and Murphy, 2017). This suggests that the redistributive effects of a pandemic do not depend solely on mortality, but on a broader range of contextual factors.
To understand this point better, consider the mechanisms that led to inequality reduction after the Black Death. First, after the pandemic, labour became scarce, real wages increased, and the poorest strata enjoyed a boost to their bargaining power and could negotiate better conditions. Second, given the partible inheritance systems (in which inheritance was shared out evenly among heirs) that prevailed in much of fourteenth-century Europe, large patrimonies became fragmented. This resulted in many people inheriting more properties than they needed or wanted, and to an unusual abundance of property being offered on the market. Together with higher real wages (indicative of lower income inequality), the situation allowed a larger part of the population to gain access to property (lowering wealth inequality as well).
The situation was not replicated after the seventeenth-century plagues. After the Black Death, when it had become clear that plague was to remain a recurrent scourge, the richest families began to protect their patrimonies from unwanted fragmentation by using specific institutions, like the fideicommissum which guaranteed that a well-defined set of family properties were transferred unaltered from one generation to the next. This interrupted one of the key mechanisms through which plague might have reduced wealth inequality. But there is more: after the seventeenth-century plagues we see no trace of an increase in real wages, either in Italy or in other severely affected European areas. Consequently, we have no reason to think that the poorest strata experienced a significant improvement in their relative income or wealth (Alfani 2020b).
The diverse long-term outcomes of the Black Death and subsequent plagues suggest the need for caution when generalising historical evidence about the impact of pandemics on inequality. Plague is also a very different pathogen compared to COVID-19. Coronavirus has much more in common with influenza, which is highly diffusible, can infect a very large proportion of the overall population, but does not have such a high case fatality rate. What can history tell us about the effects of this virus?
The 1918–19 influenza pandemic
The so-called ‘Spanish Flu’ of 1918–19 is usually taken as the worst-case scenario for a pandemic caused by a pathogen with the characteristics described above. It killed in between 2.5 and 5% of the world population (50 to 100 million victims), though the case fatality rate was quite low: 2 to 3% in most Western countries. The horrific number of victims caused by the 1918 influenza resulted from its ability to spread very efficiently: according to an estimate, it might have infected one third of the world population. This is of the utmost importance for understanding its distributive consequences. A crucial point to underline is that, compared to major plagues, the 1918 influenza did not cause a large contraction of the labour force. In other words, mortality was not high enough to lead to an improvement in the relative position of labourers – nor was it large enough to reduce inequality through a nastier mechanism: the simple extermination of the poor, which occurred both with plague and cholera pandemics (Alfani, 2020). Instead, the influenza pandemic tended to damage the income of the poorest and most fragile strata comparatively more. This is because in a pandemic which infects (but does not usually kill) a very large proportion of the population, those who need healthy conditions to work will also lose a larger part of their overall income.
Recent research suggests that the 1918 influenza pandemic led to increases in income inequality, for example in Italy (Galletta and Giommoni, 2020), for the reasons mentioned above as well as for the spread of unemployment caused by the economic crisis brought about by the pandemic. The most striking evidence, though, is for Sweden. There, for every death caused by influenza there were four new poor people who had to ask for public help at poorhouses (Karlsson, Nillson and Pichler, 2014).
What lessons for the age of COVID-19?
Epidemiologically, COVID-19 is much closer to the 1918 influenza than to medieval and early modern plagues. It can be reasonably expected that it will tend to increase, not to reduce, income inequality and poverty in each country. Indeed, many have already expressed concerns about rapidly growing unemployment, especially among the poorest, not only because of job loss due to infection but also as a result of containment policies like the lockdowns. In general, working from home proved much easier for high-income workers than for low-income ones (OECD, 2020). Consequently, if we take a long-run view and we consider all possible mechanisms through which major pandemics of the past affected distribution, we have every reason to believe that on balance, COVID-19 will increase inequality and the spread of poverty. This is also because COVID-19 will not cause enough deaths to mirror the catastrophe-induced levelling of the Black Death, which is clearly fortunate. But this means that we should start getting ready to contain, and possibly to prevent, a social crisis that will unavoidably follow the ongoing health crisis.
Guido Alfani (Bocconi University)
Further reading
Alfani, G. (2020), Epidemics, inequality and poverty in preindustrial and early industrial times, CAGE working paper no. 520 (final version forthcoming in the Journal of Economic Literature)
Alfani, G. (2021), Economic inequality in preindustrial times: Europe and beyond Journal of Economic Literature, 59 (1), forthcoming
Alfani, G., and T. Murphy (2017), ‘Plague and Lethal Epidemics in the Pre-Industrial World’, Journal of Economic History 77(1): 314–343.
Galletta, S., and T. Giommoni (2020), ‘The effect of the 1918 influenza pandemic on income inequality: Evidence from Italy’, Covid Economics, 33: 73–104.
Karlsson, M., T. Nillson and S. Pichler (2014), ‘The impact of the 1918 Spanish flu epidemic on economic performance in Sweden. An investigation into the consequences of an extraordinary mortality shock’, Journal of Health Economics, 36: 1–19.