
COVID-19: Determining trustworthiness and safety of REmote Consulting in primary Healthcare (REaCH) for chronic disease populations in Africa
Context
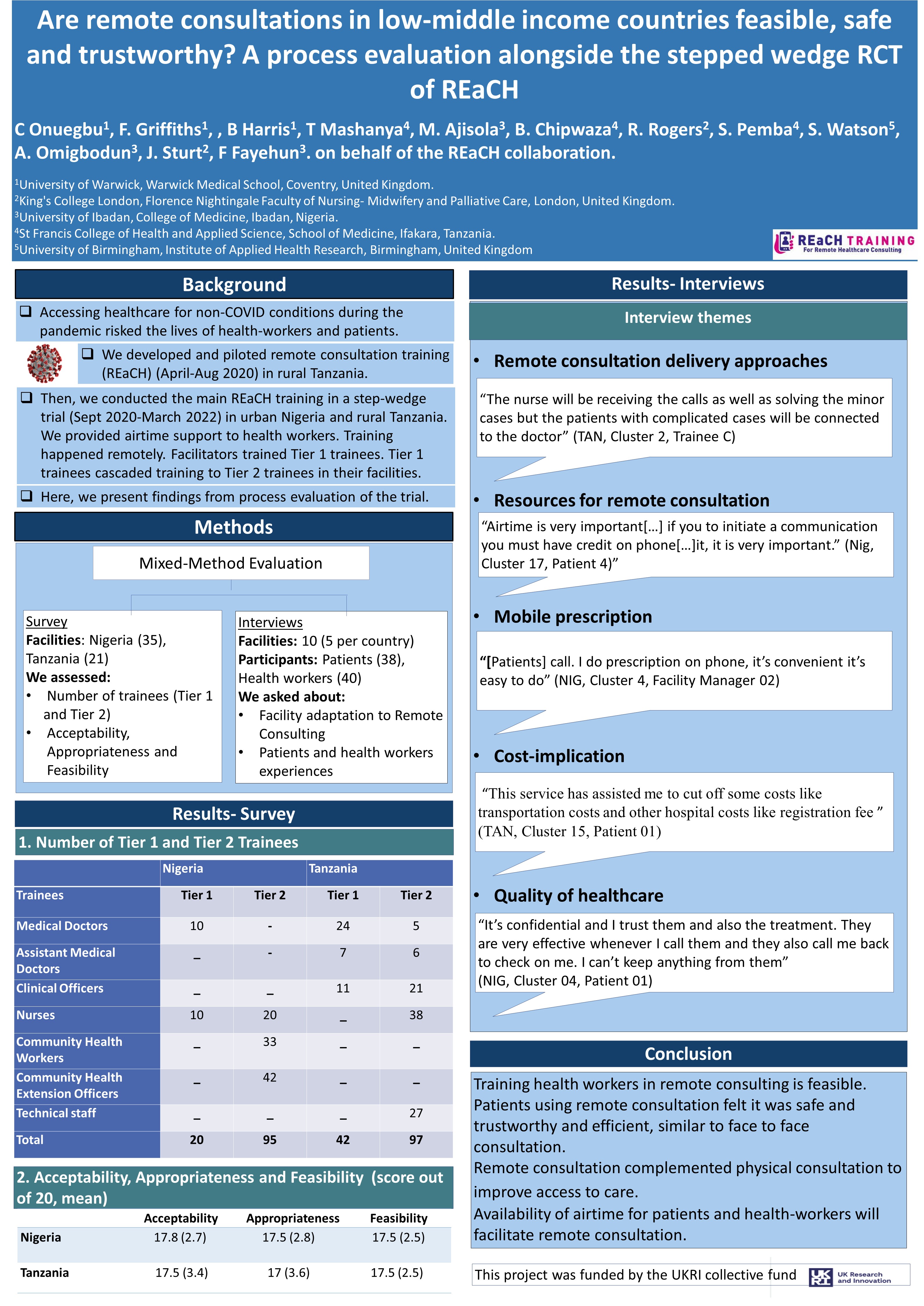
During the COVID-19 pandemic, traditional face-to-face healthcare consulting has put the world's health workforce and citizens at risk. Healthcare users often fear accessing health facilities and consequently delay seeking healthcare. To support health workers and patients to use WHO-advised, remote healthcare we have developed REmote Consulting in Healthcare (REaCH) training. REaCH optimises the limited digital/telecoms infrastructure in Africa to deliver a safe and trustworthy healthcare equivalent to face-to-face.
Tanzanian pilot
In 2018 REaCH was delivered and positively evaluated by two face-to-face cohorts of medical officers. Between April and June 2020, REaCH was digitised, delivered and evaluated by 14 Tanzanian medical officers from five primary care facilities. In response we adapted the Moodle app for stronger/weaker network capacities and made curriculum revisions.
 The Intervention
The Intervention
REaCH training is designed to increase the use and quality of remote consulting. Our training uses a blended learning Moodle app and cascade process which support the delivery of trustworthy, safe and scalable remote primary healthcare. REaCH trainees are Doctors/Nurses/Medical Officers who work for primary healthcare facilities in Tanzania and Nigeria (tier 1 trainees). They subsequently cascade training in local languages to health workers in their team (tier 2 trainees). Tier 1 training consists of 20 hours of self-directed learning plus local tutor/peer time over 2/3 weeks using a smart phone. Tier 2 training is cascaded remotely via feature phone or through locally established team meetings/training with prescribed social distancing. REaCH is informed by the TRAIN framework for optimising sustainability of changes in healthcare delivery following a cascaded learning process in LMIC.
Find out more about REaCH Training here
{kind=link}
REaCH Trials in Nigeria and Tanzania
We aim to deliver internationally unique evidence on REaCH training: whether it is effective in increasing remote consulting, whether it affects face to face consulting, and whether it changes patient reports of trustworthiness and changes specified indicators of the safety of healthcare consultations in primary healthcare.
We are running two trials in contrasting country-settings with marginalised populations: rural/remote, low income populations in Tanzania in East Africa, and urban and peri-urban middle income populations in Nigeria in West Africa.
Trial design
The trial design consists of a two stepped-wedge, non-inferiority, cluster randomised trials with nested process evaluations. A total of 56 health facilities have been recruited and divided into 40 clusters; 20 clusters per country randomized in groups of 2 to form a sequence, to receive REaCH training staggered over 12 months.
Process Evaluation
We are exploring patient and health worker experiences of remote consulting, its impact on healthcare, and enablers/impediments.
Click here to find out more about the REaCH Trials (King's College London)
REaCH Partners
Funding Acknowledgment
This project is funded by the UKRI Collective Fund: UKRI/GCRF/Newton Fund via EPSRC - COVID-funding (UK EP/V028936/1)
Additional funding supporting the development of the REaCH training includes:
- UK Research and Innovation (UKRI) Global Challenges Research Fund for Digital Innovation for Development in Africa (DIDA): Engineering and Physical Sciences Research Council (Grant ref: EP/T030240/1): Co-produced mobile consulting for remote, marginalised communities in Africa.
- King’s Together Fund: How can Remote Consulting Training for health workers in rural Tanzania be optimised to support upscaling to remote and marginalised communities of East and West Africa?
Nurturing collaboration: South-South and South-North
Running alongside the Trials, our multi-disciplinary team is sharing experiences and lessons about remote consulting in Uganda, Kenya and the UK.