
Elective report - Porto Alegre
An Elective in the John Ernsting Aerospace Physiology Laboratory, Micro G, TECNOPUC, Pontifical Catholic University of Rio Grande do Sul, Porto Alegre, Brazil.
Introduction
I undertook my elective at the John Ernsting Aerospace Physiology Laboratory, Micro G, Pontifical Catholic University of Rio Grande do Sul (PUCRS), Porto Alegre, Brazil under the supervision of Professor Thais Russomano. I spent the majority of my time in the laboratory and was fortunate enough to visit surrounding hospitals and be involved in various projects the laboratory undertook. Through my time in Porto Alegre I was able to learn about various differences in healthcare systems, as well as being able to interact with a vast range of specialists in which aerospace medicine plays an important role in their everyday activities from sports scientists to pilots.

Objectives
Proposed learning outcome of the elective:
1. Experience the unique speciality of aerospace medicine
2. Improve knowledge regarding human physiology in extreme conditions (e.g. micro gravity)
3. Gain a publication within this field
4. Gain experience in lab based research
5. To understand and adapt to the multi-cultural and multi-disciplinary academic team environment
6. To create and follow through a reach idea of my own from protocol stage through to definitive conclusion
Porto Alegre
Culture of the Gaúcho
Gaúcho is the main demonym of the people from the state of Rio Grande do Sul that Porto Alegre is situated within. I found the people of Porto Alegre to be delightful people, who were very warm, friendly and welcomed me with open arms.

Healthcare
Porto Alegre and its hospitals
Porto Alegre (Joyful Harbour) is the capital and largest city in the Brazilian state of Rio Grande do Sul and is the tenth most populated city in Brazil. Life expectancy of the Brazilian population is 74.6 years from 2012 data and according to predictions will catch up to the current leaders in life expectancy by 2040 [2].
The national health policy of Brazil is similar to the NHS and is based on the Federal Constitution of 1988, which created the Sistema Único de Saúde (SUS) where those who are unable to pay for health care utilize the SUS. Roughly 30% of the population utilizes private healthcare through insurance and health plans. Compared to the UK, there are some not for profit private hospitals that reinvest their entire profit back into the SUS, the majority of funding however comes from taxes and business profits which is given to 26 regions across Brazil, each of which decides how to spend it (similar to the now obsolete PCTs in the UK). The total expenditure on health per capita is $1,109 which is 9.3% of the GDP, compared with the UK’s $3495 and 9.4% [3].
Currently ischemic heart disease is the largest killer in Brazil accounting for 10.5% of deaths in 2012, followed by stroke, lower respiratory tract infections and diabetes [4]. This is a different picture compared to the UK’s current leading causes of death: Ischemic heart disease, Stroke, Tracheal, bronchial, lung cancers and Alzheimer’s [5].
Through connections Prof Russomano had with various health professionals in Porto Alegre I was able to visit the local university hospital as well as a private radio-oncology hospital and gain an insight into the functioning of healthcare in Brazil. The local hospital was similar in care standards to the UK, however it was exceptionally crowded and had incredible waiting times, (over a year for radiotherapy for various cancers), compared to the UKs 2 week wait initiatives. Additionally healthcare was of a very paternalistic model in these hospitals. The private hospital on the other hand was beyond NHS standards, all facilities were immaculate, scans were done on the day, treatment started within days of diagnosis, hospital food was exemplary, minimal waiting times, incredible restaurants and even a waterfall in the lobby! Unsurprisingly healthcare here was more of a partnership between clinician and patient.
What is Aerospace Medicine?
Aerospace Medicine, is an evolving multi-disciplinary it is dedicated to enhancing health and safety in those who work or travel in the aerospace industry from commercial to military air travel all the way to the sub speciality that interests me the most, space travel [6]. Microgravity experienced in space provides a very unique set of health problems:
• Space adaptation syndrome (SAS) which is essentially space motion sickness [7].
• Loss of bone mass (due to alterations in osteoblast and osteoclast activity) and muscle mass (due to inactivity) all arising from the absence of gravity [8].
• Fluid redistribution is a significant issue in microgravity, it ultimately reduces the circulating fluid resulting in cardiac atrophy, additionally re-entry back to 1G causes orthostatic intolerance [9].
• Visual impairment due to intracranial pressure (VIIP) is of interest to me given my background in optometry, as the name suggests it is due to suspected effects of intracranial pressure on the eye, this is currently the biggest barrier to long term human space flight [10].
• Psychological effects are also significant in space due to sleep disruption, emotional disruption, stress and isolation. There has also been recent concern about spaceflight accelerating the onset of Alzheimer’s disease [11].
Micro G Laboratory
The Micro G was originally built due to political interest Brazil originally generated when it was a bilateral partner of the USA to supply hardware to the station. The principal activities of the laboratory are the development of research projects focused on: biomedicine before, during and after simulations of hypergravity, hypogravity, microgravity and parabolic flights, aerospace biomedical engineering and eHealth.
One of several interesting cultural differences was the absence of a significant barrier between lecturers, professors, doctors and students as is in the UK. Regularly academics and students would go for lunch together and there seemed to be less of a gulf between provider of knowledge and student, providing many opportunities for the exchange of ideas and richer learning beyond a rigid syllabus. There was also a relaxed approach to time keeping, many meetings happened hours after their agreed start time, at first this appeared rude but I quickly realized it was merely cultural, it highlighted to me the subtle and unspoken differences in culture ever important to be aware of when working in a team.
Academic Activities
Physiological aspects of Walking in Simulated Hypogravity
As part of my time at the Micro G laboratory I was fortunate enough to be able to take over a project that was investigating the physiological aspects of walking in simulated hypogravity.
Understanding the biomechanics and energetics of walking in a hypogravity environment has recently received renewed interest with projects such as the possible manned missions to Mars [12]. We know that hypogravity environments result in a significantly altered gait to terrestrial based gaits, as well as alterations in metabolic energy requirements for locomotion. The challenge is further studying this and trying to understand the reason for these altered energy requirements. I was privileged to be able to use this as an opportunity to expand my knowledge in aerospace physiology and was required to do a significant amount of learning around human gait and the mechanics behind body suspension devices (BSD), these devices partially sustain the individual’s weight.
It is through this that we intend to study the differences in gait between normo gravity (1G), lunar (Lunar G) and Martian (Mars G) based ambulation. The data had been collected from 9 volunteers from the university, these volunteers were placed in a BSD and had baseline VO2 measured using a mask that was placed over the volunteer’s nose and mouth and heart rate (HR) was measured using a cardiotachometer that was adjusted around the chest. This was also combined with measures of comfort, pain and exertion.
The BSD was then engaged and the volunteers underwent 10 minutes of walking at a self-selected speed, in a simulated Mars G environment, followed by a rest period to baseline HR. A lunar environment was then simulated for another 10 minutes walk, followed by a walk at 1G for 10 minutes.
The results of this were that as gravity is decreased self-selected walking speed decreases and as expected any level of activity beyond rest increases the heart rate. However, there was no significant difference in HR between altered Gs. Metabolic activity as shown through relative and absolute VO2 was found to be significantly different between rest and 1G, however again no difference was found between the other levels of hypogravity. This originally presented quite a confusing set of results as it was expected HR and metabolic rate would vary together and proportionally. This prompted myself and Prof Russomano to bring together various members of the team including physiologists and engineers to discuss why these changes occurred, together we had many different ideas. After much reading around the subject and with the stimulation from discussions with my colleagues my hypothesis as to this outcome is the possible influence of the skeletal muscle pump working in mechanically simulated hypogravity, but the vascular system is functioning within 1G as the BWS does not alter the effect of gravity on the blood, only on the mechanical work required by muscles. This would result in a reduced cardiac pre-load which would cause an increase in HR, this would work in concert with the autonomic component of the pain response from the harness to increase HR. It may therefore be that the combination of the above factors along with the self-selected speed that reduced the change in VO2 to below significance.
I was able to apply my own knowledge gained through medical school and build upon it which allowed me to identify some key points within the study:
• Small sample size, with an uneven split between the genders.
• Communication difficulties with the researchers performing measurements resulted in the first three volunteers having spurious data points which required their removal from the data set. This was a valuable lesson of not only language barriers, but ensuring the entire team understands the need for consistency in data collection.
• Confounding factors in the Borg scale was introduced by discomfort from the harness, lack of unloading above the torso and reduced freedom of movement.
• Finally a BWS will always be limited when studying cardiovascular function in hypogravity due to its inability to truly affect cardiac pre-load and after-loading as true hypogravity may.
For the next part of this study I observed data collection this time looking at a lower body positive pressure device (LBPP), this time including surface electromyography and the calculation of the Froude number, (the ratio of Centripetal force to Gravitational force during walking), which through my review of current literature may show some interesting alterations in gait due to the similarity human gait has with an inverted pendulum. The data is still being collected from PUCRS student volunteers and I will be writing this up for a second paper later this year.
Publications
I have from this experiment produced a poster which has successfully been accepted at the 20th Humans in Space symposium in Prague the end of June (see Appendix 1) as well as a paper which is currently under review for the Life Sciences in Space Research journal. As well as a poster shown at a local conference held at the university hospital attached to PUCRS which I created along with a student I met at the medical school, they translated the poster and I wrote the content.
As part of my time spent at Micro G I became very familiar with the effects of hypogravity on gait and due to this wrote a presentation for my professor to present at the Aerospace Medical Association (AsMA) 2015 conference in Orlando 2015. This is the largest aerospace medicine conference in the world which provides a forum for all aerospace medical disciplines from civilian, military and private sectors.
This presentation was based on a literature search looking at locomotion in hypogravity and summarized 6 studies using a BWS device [13-18], 4 studies which used a lower body positive pressure (LBPP) box [19-22] and 1 study which used a parabolic flight [23].
The results of my literature search showed the following key points:
• Running is more energy efficient in hypogravity than walking, as is the case on earth.
• We currently do not know where excess energy is being expended in the hypogravity affected gait cycle
Participation in International Collaboration
I was incredibly fortunate that during my time at the Micro G Professor Russomano took me under her wing and showed me significant insights into the day to day running of the department. I was able to observe Prof Russomano providing leadership in research, both nationally through various projects such as the tele-medicine project, but internationally by building connections with Lisbon and Venezuela in their respective aerospace laboratories and I was able to take part in these meetings and contribute. It was fascinating to be exposed to university governance and management, which I would otherwise never be able to have appreciated.
My original elective plan to Micro G was to include doing my own original research looking at an automated chest compression device called LUCAS, this device has been used in the emergency services in the US, Sweden and Germany for several years now [24].
On Earth we use our weight to perform CPR, but space prevents us doing this, depending more on strength. Additionally due to Newton’s laws of motion each compression will propel the rescuer in the opposite direction! Various techniques to counter this in microgravity have been developed [25] all of which involve the rescuer wrapping their body around the patient.

The LUCAS device however has never been investigated in microgravity, the benefit of having an automated device providing chest compressions would allow a rescuer at the scene to be able to provide rescue breaths or other lifesaving activities instead of physically exhausting chest compressions. The Micro G laboratory has close contacts with a laboratory in Lisbon which has a specialist interest in cardiology and has agreed to collaborate with the Micro G. This will involve a Resusci Annie and a BWS to measure the efficacy and fatigue over time of a LUCAS device compared to a human rescuer performing CPR. I am currently in the process of re-writing the study protocol for submission.
Giving Lectures
I was fortunate enough to be offered the opportunity to provide a lecture to the students engaged with Micro G, my audience was comprised of many specialities from medicine and engineering to physics.
I spoke about the UK healthcare system as well as medical education in the UK and how it differed, as well as my research at the Micro G. I followed this with a group discussion regarding the results of my project which provided a very stimulating and lively discussion!
Telemedicine
As humans travel further into space, it will be impractical to provide local healthcare, therefore the integration of telecommunications and medical technologies is essential. An underappreciated part of aerospace medicine is bringing technology back down to earth after development, and as part of this the Micro Gs is dedicated to performing ongoing work in tele-medicine.
Dermatology Clinics
I was able to attend several telemedicine clinics held in Centro De Extensao Universitaria – Vila Fatima, which was an outreach clinic in an impoverished area in an adjacent town. The purpose of these telemedicine clinics was to work in collaboration with the computer science department as well as the medical school to both refine the IT system and to also serve as an introduction for the medical students into the field of telemedicine, as part of an initiative to reduce resistance and uptake of telemedicine systems in the future.
This ongoing tele-medicine project is focusing on dermatology clinics in Vila Fatima, the current clinic stream is as follows:
• The patient registers attendance.
• History and examination performed by medical students and provisional diagnosis and management reached.
• Data entered on telemedicine database including photographs of skin.
• Patient is reviewed by consultant and management initiated.
• Patient data is collated and reviewed and audited to assess function of system and conformity of diagnosis and management.
Logistical planning of a large telemedicine project in rural area
My time at MicroG also allowed me to participate in the logistical organization of a telemedicine project that was a joint project between PUCRS and the Municipal Secretaries of Health and Culture for Rio Grande do Sul to help bring cardiology services to remote regions of Rio Grande do Sul. This required me meeting with various clinic managers and doctors to help plan required equipment and translators for the plan which was being performed in collaboration with Kings College London.
Other Activities
I was also fortunate to receive a flying lesson from a commercial pilot from the aeronautical sciences department, needless to say my first ever landing left something to be desired!
I was able to observe filming with a Brazilian television crew covering Brazil’s contribution to space flight and I was honoured to meet Professor Thaisa Bergmann, an astrophysicist who has recently won the L’Oréal-UNESCO Women in Science Award 2015 for her work on the evolution of galaxies and the effect super-massive black holes have on them [26]. As well as meeting an astronaut selected for the Mars One 2020 project [12].
Conclusion
My work in the Micro G has provided me with unique knowledge that I would never have been able to acquire anywhere else, and has additionally provided me with an entry point into aerospace medicine. The insight into the running of laboratories and day to day activities of a Professor were also enlightening to see, and it was a great experience to work with so many different specialties each looking at a different piece of the puzzle.
The differences in healthcare differences between Brazil and the UK were interesting to note and while in developed cities these differences were very small, in rural areas that I visited they were drastic. Brazil really struck me in its dichotomy between the wealthy and the poor that was evident everywhere.
I believe I have invaluably furthered my experience in medicine, gaining both clinical knowledge and significant theoretical knowledge surrounding human physiology and space, as well as experience in designing, carrying out, analysing and writing up research which I will be able to take forward with me as I enter into my final year of medical school and beyond. As healthcare in the UK and the world continues to change I feel the insights I have gained will prove valuable in accepting the necessity for input from many specialties along with ongoing integration with IT services.
I have learnt the importance of clearly communicating research protocol to people who will be participating in research studies and the issues the language barrier may play in this when working internationally, as well as the importance of cooperation with different specialities and students to help push research forward.
I am very pleased to say that I fulfilled my original elective objectives, with ‘Objective 3’ still pending acceptance into the journal for publication and I am very excited to move forward with ‘Objective 6’ along with Lisbon which will hopefully develop further through the year.
As it is clear to see Aerospace medicine is a truly fascinating subject which is rapidly developing and as unrealistic as it may seem I believe assuming humanity survives long enough, it is our destiny to leave the planet and explore the stars. I am incredibly honoured to have been able to participate in research that will one day – in a very tiny way - help humanity in this endeavour.
Acknowledgements
My time in Porto Alegre has taught me many things, given me many life lessons that are inexpressible in their value and provided me with many experiences. For this I am grateful to the Entwistle Fund for providing £400 without which I would not have been able to embark upon my elective in the first place.
References:
1. Control, P. LUCAS Device. 2011; Available from: http://www.lucas-cpr.com/.
2. (IBGE), B.I.o.G.a.S., BRICS: Joint Statistical Publication 2014. 2014: Instituto Brasileiro de Geografia e Estatística - IBGE.
3. WHO. WHO: Country health breakdown. 2012; Available from: http://www.who.int/countries/bra/en/.
4. WHO. Brazil: WHO Statistical Profile. 2012; Available from: http://www.who.int/gho/countries/bra.pdf?ua=1.
5. WHO. United Kingdom: WHO Statistical Profile. 2015; Available from: http://www.who.int/gho/countries/gbr.pdf?ua=1.
6. Dehart, R. and J. Davis, Fundamentals of aerospace medicine: translating research into clinical applications. 2002, United States: Lippincott Williams And Wilkins. p. 720.
7. Homick, J., M. Reschkle, and J. Vanderploeg, Space adaptation syndrome: incidence and operational implications for the space transportation system program. 1984, DTIC Document.
8. LeBlanc, A., et al., Bone mineral and lean tissue loss after long duration space flight. J Musculoskelet Neuronal Interact, 2000. 1(2): p. 157-60.
9. Buckey, J., et al., Orthostatic intolerance after spaceflight. Journal of Applied Physiology, 1996. 81(1): p. 7-18.
10. Otto, C., et al., PROSPECTIVE OBSERVATIONAL STUDY OF OCULAR HEALTH IN ISS CREWS–THE OCULAR HEALTH STUDY.
11. Cherry, J.D., et al., Galactic cosmic radiation leads to cognitive impairment and increased aβ plaque accumulation in a mouse model of Alzheimer's disease. PloS one, 2012. 7(12): p. e53275.
12. MarsOneTeam. Mars One. 2013; Available from: http://www.mars-one.com/.
13. Farley, C.T. and T.A. McMAHON, Energetics of walking and running: insights from simulated reduced-gravity experiments. Journal of Applied Physiology, 1992. 73(6): p. 2709-2712.
14. Margaria, R. and G. Cavagna, Human locomotion in subgravity. Aerospace medicine, 1964. 35: p. 1140-1146.
15. Griffin, T.M., N.A. Tolani, and R. Kram, Walking in simulated reduced gravity: mechanical energy fluctuations and exchange. Journal of Applied Physiology, 1999. 86(1): p. 383-390.
16. Grabowski, A., C.T. Farley, and R. Kram, Independent metabolic costs of supporting body weight and accelerating body mass during walking. Journal of Applied Physiology, 2005. 98(2): p. 579-583.
17. Leães, R., et al. Development of walking pattern evaluation system for hypogravity simulation. in Engineering in Medicine and Biology Society, 2006. EMBS'06. 28th Annual International Conference of the IEEE. 2006. IEEE.
18. Hurd, W.J., et al., Differences in normal and perturbed walking kinematics between male and female athletes. Clinical Biomechanics, 2004. 19(5): p. 465-472.
19. Cutuk, A., et al., Ambulation in simulated fractional gravity using lower body positive pressure: cardiovascular safety and gait analyses. Journal of Applied Physiology, 2006. 101(3): p. 771-777.
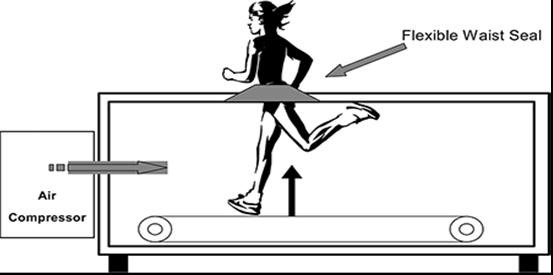
20. Grabowski, A.M., Metabolic and biomechanical effects of velocity and weight support using a lower-body positive pressure device during walking. Archives of physical medicine and rehabilitation, 2010. 91(6): p. 951-957.
21. Buono, M.J., et al., Alterations in the Rate of Limb Movement Using a Lower Body Positive Pressure Treadmill Do Not Influence Respiratory Rate or Phase III Ventilation. BioMed research international, 2015. 2015.
22. Patil, S., et al., Anti‐gravity treadmills are effective in reducing knee forces. Journal of Orthopaedic Research, 2013. 31(5): p. 672-679.
23. Cavagna, G., P. Willems, and N. Heglund, The role of gravity in human walking: pendular energy exchange, external work and optimal speed. The Journal of Physiology, 2000. 528(3): p. 657-668.
24. Olsson, P., et al., The outcome of cardiac arrest the years before and after introduction of LUCAS in the ambulances. Resuscitation, 2008. 77: p. S9.
25. Rehnberg, L., et al., Three Methods of Manual External Chest Compressions During Microgravity Simulation. Aviation, space, and environmental medicine, 2014. 85(7): p. 687-693.
26. Storchi-Bergmann, T., et al., Nuclear spirals as feeding channels to the Supermassive Black Hole: the case of the galaxy NGC 6951. The Astrophysical Journal, 2007. 670(2): p. 959.